

A/ ALZHEIMER a neurodegenerative disease.
Alzheimer's disease causes memory and behavioural disorders in the individual. It starts in a banal way, with small omissions, confusions about everyday things (time, places, events etc....), but gets worse as the brain deteriorates. The progression of the disease is not uniform from one patient to another, it is estimated that the average life expectancy after the onset of symptoms is eight years. There is currently no treatment to stop the progression of the disease, but some drugs are available to treat the symptoms of dementia. Over the past thirty years, research on dementia has led to a deeper understanding of how Alzheimer's affects the brain. Today, researchers continue to look for more effective treatments and a cure for the disease, as well as ways to prevent its onset and improve brain health (source- Alzheimer org). The origin of this disease is not yet clearly identified, it affects all social classes without distinction of race or sex (although it more often affects women).
Discovered in 1906 by Aloïs Alzheimer, Alzheimer's disease is a brain disorder called "neuro-degenerative", i.e. it causes a progressive disappearance of neurons. More than 100 years after the discovery of Alzheimer's disease, the causes of this complex neurodegenerative pathology are still not precisely known.
To put it simply, and understandable to everyone, neurons are cells of the nervous system, specialized for communication, and information processing (listening, reading, understanding, reflecting, thinking, feeling etc...). Thanks to neurons, we can achieve and accomplish things, simple (listening, answering, etc.) or complex (discussing, reasoning, working, etc.). Over time, the neurons become exhausted and disappear. This gradual reduction or disappearance leads to an alteration of our intellectual and cognitive faculties (language, memory, reasoning, behaviour, etc... and even motor skills. The patient loses the sense of orientation, in time and space, and then difficulties with language, and even visual recognition of things, of close people. This leads to a progressive and significant reduction in the autonomy of the person concerned. And created a situation of dependency.
This disease is not a normal consequence of ageing, it affects women a little more often than men, and more rarely under the age of 60, even if cases have already appeared, for subjects as young as 50. (France Alzheimer)
Neurofibrillary degeneration is the appearance, within neurons, of abnormalities in the Tau protein;
Amyloid plaques or "senile plaques" are the deposition, outside the neurons, of the amyloid beta protein.
These lesions gradually invade the different areas of the cerebral cortex. They are silent for a long time and then cause visible manifestations as they multiply and affect areas important for brain function.
ALZHEIMER'S DISEASE BEGINS IN THE HIPPOCAMPAL REGION: THE MEMORY AREA OF THE BRAIN. (France Alzheimer)
In this first phase of the disease, about 25% of the hippocampus decreases in volume. The neurons in the area dealing with the link between short-term and long-term memory are partially damaged, so the person's memory capacities are slightly diminished: they have minor oversights of recent names or events and have difficulty acquiring new information. Short-term memory disorders increase as the hippocampus continues to lose neurons and causes difficulties in organizing daily life.
Over time, several other areas of the brain are in turn damaged, particularly in the temporal-parieto-occipital associative cortex, resulting in disorders of gestures, language and recognition. (France Alzheimer)
At an advanced stage of the disease, as brain damage has progressed, information retrieval can hardly be done anymore, the person forgets the events and information of his past.
Warning signs
Loss of sense of time, frequent mood swings, forgetting recent events, difficulty recognizing some people, what are the first signs of the onset of Alzheimer's disease?
Even if they are not necessarily related to Alzheimer's disease, some signs must be alerted, especially the following 10 signs:
1 - Memory loss
The person increasingly forgets recent events affecting his or her personal life and surroundings but keeps a very good memory of past memories.
2 - Difficulties in performing daily tasks
The person encounters difficulties to carry out familiar tasks such as preparing a meal, shopping, managing the expiry dates of food in the refrigerator....
3 - Language problems
The person no longer finds simple, everyday words and uses others that are more or less appropriate.
4 - Disorientation in time and space
The person's sense of orientation decreases. It can get lost, even in familiar places, and confuse the seasons. (France Alzheimer)
5 - Difficulties in abstract reasoning
The person has difficulties with administrative formalities, managing their finances (especially from the euros), writing a cheque, calling someone on the phone.
6 - Loss of objects
The person tends to place objects in unusual places (a watch in the oven) without ever finding them.
7 - Alteration of the judgment
The person can no longer assess the situations: he or she wears winter clothes in summer, makes excessive purchases of food...
8 - Behaviour modification
The family and friends notice the appearance of a depressive tendency in the person or manifestations of anxiety, irritability, agitation....
9 - Loss of motivation
Motivation falls for all activities, including those that were once a passion.
10 - Personality change
The person becomes completely different from what he or she was and loses his or her own character: jealousy, obsessive ideas of prejudice, excessive exuberance...
Cognitive symptoms
Alzheimer's disease is not just about memory disorders, even if they are the first to appear. The evolution of brain damage gradually prevents other abilities from functioning.
Memory disorders
The first disorder that appears in Alzheimer's disease mainly concerns episodic memory (forgetting recent events, appointments, no longer knowing how to find your way around a familiar city, etc.). (forget recent events, appointments, no longer knowing how to find your way around a familiar city, etc.).
But Alzheimer's disease also affects the person's other memories:
The memory of work that allows us to retain information in the immediate future to keep it at our disposal in order to quickly solve problems, organize our speeches, and make decisions;
Long-term memory, the essential purpose of which is to keep information for a long time. It is the damage to this memory that causes the sick person to not know where he or she is or how he or she came, to lose his or her bearings until he or she no longer finds himself or herself in the home, and to disrupt his or her ability to create new memories and record new knowledge,
Semantic memory , which corresponds to the memory of concepts, of the knowledge we have about the world, of our cultural background.
.Procedural memory, which is expressed in a person's motor activity. It is memory that allows the progressive acquisition and retention of skills.
Language disorders
After memory disorders, language disorders, or aphasia, are the most important. They correspond to a partial or total loss of the ability to communicate, and therefore affect the ability to understand language and/or speak.
The inability to speak develops in successive stages:
first the vocabulary is reduced, the person searches for words,
then the person uses only one word or sound, whether it is in several tones or speaks a lot in jargon that makes no sense.
If comprehension is preserved longer than expression, however, the ability to understand language gradually decreases. At first, they are complicated sentences or a precise vocabulary that seem obscure to the patient, then at the end of the evolution simple sentences and basic words will also become incomprehensible.
Gesture disorders
The patient is in the incapacity to perform actions that he has acquired throughout his life. This learning of gestures will gradually disappear. This will involve complicated actions such as writing, eventually occurring even for simple gestures, such as chewing or swallowing food.
It is this disorder that will cause a great loss of autonomy and will require assistance for bathing, dressing, cooking, etc. The extent of the deterioration of these abilities is different for each person, some will quickly become very difficult in their daily lives, while for others there will always be a minimum of skills. (France Alzheimer)
The psychological aspects of the disease
The origin and risk factors
While researchers have clearly identified the mechanisms of lesion production, they have not yet identified the causes of their appearance. However, researchers have identified circumstances that favour the development of Alzheimer's-type diseases, which are linked to genetic predispositions and multiple environmental factors, known as "risk factors".
<Among these "Risk factors are:
age: the elderly are the most affected;
sex: the risk of developing the disease is higher in women after 80 years of age;
vascular risk factors;
diabetes, lipid disorders, high blood pressure, and tobacco;
family history: However, the so-called "family" forms of the disease only affect about 1% of all sick people.
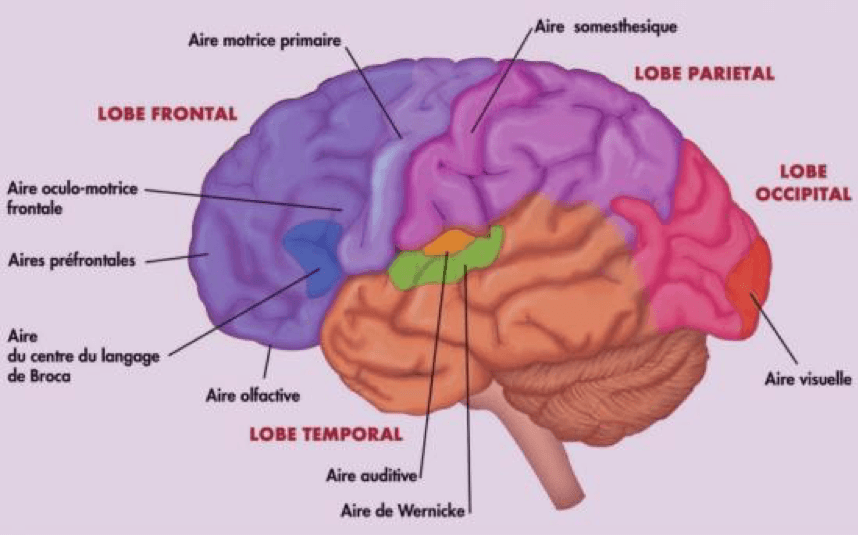
The hippocampus and temporal lobe
The hippocampus processes verbal memory (memories associated with what we have read, said or heard) and visual memory (recognition of objects, faces, places). The temporal lobe controls recent learning and immediate memory. The hippocampus and temporal lobe represent the centre of memory and language.
The parietal lobe
It allows us to perform tasks or use tools in a coherent and logical order (such as putting on clothes in the right order, starting and driving a car, etc.) It also controls our ability to understand spatial information (for example, the precise location where we are, the location of places, objects). (France Alzheimer)
The frontal lobe
It allows us to take initiatives, to plan to organize our actions. It controls our values and our behaviour in society.
The occipital lobe
It controls vision, the ability to see and associate colours, shapes, angles and movements in an intelligent way. Although this lobe is not directly affected in Alzheimer's disease, the neighbouring visual areas that allow us to associate the elements of vision can be affected, resulting in perceptual disorders.
The psychological aspects of the disease :
Denial
Denial is a psychological defense mechanism that is not controlled. It may be total, the sick person or those around him or her denies reality, but more often than not, it is only partial. In this case, people are able to reason around the disease, but on some points, they act as if there is no disease. Shock and denial belong to the same group as denial.
Anger
Frequently, before being able to fully consider the reality of the disease, the sick person or their loved ones will go through a phase of anger against what is happening. It is a way to fight against a painful reality. This is often a stage where you are looking for a manager. It is at this time that there are the most conflicts, even ruptures, within the family or friendly group. It is also expressed to the medical community, where real elements of dissatisfaction will be added to this anger.
Guilt
Guilt is specific to the sick person's relative. Anger, following the awareness of the disease, is also a time when the events that occurred before the diagnosis are illuminated with another meaning. By better understanding the inconsistencies and previous behaviours of the sick person, the relative returns to his or her own attitudes, blames himself or herself for having acted wrongly, for not having understood. There may then be a very strong sense of guilt.
Depression
The next step is accompanied by depression. While this is often a difficult step, it is necessary and even healthy. It's normal to be sad, to be resigned. The sick person or their loved ones may want to cry or need to talk about what is happening to them, to understand, to give meaning to this ordeal.
Acceptance
The last step, which not everyone achieves, is called acceptance. It is a term that can be confusing and confusing to those closest to it. This is not about giving up. It is about being able to recognize that the disease is there, that it is no longer possible to do "as before" and that we have no choice but to "deal with" it.
This is when the family and friends will be able to adapt, better organize themselves to support the sick person. The pain, the difficulties are still there, but we can face them with all our judgment and reasoning skills.
Psychological support
The psychological impact of the disease is often violent, whether for the sick person himself, for his closest carer or for his family as a whole. To best achieve the "acceptance" stage, it is therefore not necessary to hesitate to seek the support of a professional third party, and more particularly a psychologist.
(Sources: France Alzheimer.)
Living with disease
Because of lack of knowledge, people tend to reduce the disease to its most disabling phase. Do not let yourself be influenced by certain negative representations of the disease. Just because you are sick does not mean that your life stops.
You must stay active as much as possible, while recognizing your limitations: you will have to adapt your activity level according to the progression of the disease. Some tips will be useful for some, useless for others. It is up to you to find your rhythm and your way of being an actor in the disease.
Communicate
Due to illness, communication with others may change. Your loved ones may get angry and angry at your forgetfulness. Some will even blame you for not making an effort and put you in situations that look like tests. Some friends or neighbours may avoid you, often because they are unfamiliar with your condition and afraid of not knowing how to handle it. Your relationship life may also be weakened, as everyone's roles are modified. All this means that you may tend to withdraw into yourself, yet it is essential to continue to associate with your family and friends.
What can help you
Family often wonders how you are coping and how to help yourself. Whenever you feel it is necessary, tell them about your problems, especially your memory problems.
The onset of the disease is also an emotional shock for those around you. Organizing a family meeting can be a good opportunity to talk about it. However, choose your contacts carefully, some people around you will be more comfortable than others.
Feel free to ask for help. Informed people can be very understanding and even feel valued for being able to help you.
Communication does not stop at words. If necessary, use gestures, facial expressions, voice intonations to make yourself understood.
Don't keep your grandchildren away, just explain to them what characterizes your illness. There are several books that tell the story very simply.
Be inventive
There are many tips to avoid memory failures and make your life easier. Doctors talk about "compensation strategies".
What can help you
Use a calendar that you will keep with you at all times and in which you will write down:
- important numbers, including yours and those to use in an emergency ;
- the names of people around you ;
- a map of your neighbourhood showing the location of your home ;
- a list of things to do ;
- your appointments ;
- any ideas or thoughts you want to remember.
Write down your ideas before making a phone call.
Use a calendar, to remind yourself of the date and note important events. Ask your family or a friend to call you to remind you of the time of a meal, appointment or medication. For the latter, a pill dispenser (sold in pharmacies) may be useful.
Label the cupboards with words or pictures, for example: crockery, table linen, socks, etc., if necessary.
Reorganize your closets to make it easier to choose clothes and so that you don't have to use a stool or step stool.
Use a reminder to remember, for example, to "close the stove" or "unplug the iron". If possible, use electrical appliances with automatic shut-off devices and install a smoke detector.
Ensure that you have good lighting, especially in corridors and stairs.
Stay active
Don't let apathy win you over. It is important to keep a regular rhythm of activity, to maintain both physically and morally. (France Alzheimer)
Physical activities
Gardening, crafts, walking, jogging, football, cycling, swimming, flexibility, weight training or balance exercises... any physical activity is good. Also think about relaxation, meditation and deep breathing exercises, such as yoga. In addition to staying in shape, these activities help to reduce the stress that doctors suspect is a contributing factor to the worsening of the disease.
Intellectual activities
Like the body, the mind needs exercise. This intellectual stimulation can take a playful form: letter games (scrabble, crosswords), question games (Trivial Pursuit), reasoning games (dominos, puzzles), skill games (mikado), strategy games (Monopoly), construction games (models)...
Social and cultural activities
Go to the cinema, the theatre, conferences, continue reading books are also possible activities. If you enjoy reading less, you can still listen to recorded books. You can also engage in a writing activity: emails, letters, postcards, diaries... If writing is difficult for you, you can ask a relative to write what you dictate. You should also know that there are computer programs that can transcribe your words. Don't neglect musical activities, concerts, listening to records, music therapy.
Of course, you must make sure you stay in touch with yourself and keep a pace that suits you. Over time, you may need to adapt your activities. Your abilities are not the same whether you are in the early or moderate phase of the disease.
In general, be tolerant towards yourself:
Allocate yourself a lot of time, don't let others rush you. Try to find quiet and quiet environments.
If you have any omissions, don't focus on them and move on.
If there are activities or tasks that you find complicated, get help to simplify them.Be careful to do only one
All generations combined
In schoolyards, high schools, at work with colleagues, at home with family, the word Alzheimer is often present in conversations, either seriously or in the tone of a bad joke.<Sick people quickly tend to move away from reality, these new ways of exchanging "reconnect" them and allow them to better integrate themselves into social life. The elderly are no different from us, they need to be looked at, to exchange, to express themselves. The ability of children to maintain ties beyond social norms and codes is a real asset that reduces the marginalization of people with Alzheimer's. At the same time, the contribution of patients is also important for everyone, they have been actors in the collective and family history, and are even more so.
(France Alzheimer)
On the other hand, children's tolerance and curiosity capacities have a positive impact on the self-esteem of sick people and allow them to stimulate, in a different context, their cognitive functions.
The advantages of intergenerational exchanges are therefore multiple and above all reciprocal. However, setting up a real intergenerational project is not easy, because it is not just a matter of bringing two generations together in the same place. For the impacts to be beneficial, the exchange must be based on a common project.
To support you in your care:

The primary caregiver is the family member who spends the most time caring for and accompanying the sick person. When present, the spouse usually plays this role. In the absence of a spouse, it is most often a child of the sick relative who assumes this responsibility. However, it is useful to identify other family members, sometimes even neighbours or friends, directly or indirectly involved in the support, who can play an equally important role with the person.
The impact on daily life
When you accompany a parent with Alzheimer's disease or a related dementia, you find yourself a little, despite yourself, engaged in a helping relationship that necessarily changes the nature and often the quality of the relationship established beforehand with him. For the primary caregiver, it is a matter of meeting the growing needs of the sick person and adapting assistance as the disease progresses. One can quickly be destabilized by these changes and powerless to adopt the right attitude.
Maintaining a social life
For lack of time, fear of the sick person's behaviour, shame of others' eyes, the caregiver can quickly reduce his relational life and gradually desocialize himself. An exclusive relationship may then develop between the caregiver and the person being cared for, a kind of double confinement, where it is considered that the patient's loved one must be overprotected and the caregiver's existence is gradually reduced to the exclusive care of the sick person.
Agree to be helped
The daily support of a sick loved one is fraught with consequences. In order to avoid physical and psychological exhaustion, the caregiver must be able to identify the external resources available in his or her environment and identify possible responses to the needs of the sick person. (France Alzheimer)
These relays are to be found in the family, friendly and neighbourhood environment, but also with care professionals, home help and also day hospital and day care facilities. Meals are often moments of sharing within families that are shaken up by the arrival of the disease. Eating disorders and the disorganization of meals they cause can quickly lead to misunderstanding between you and the sick person. Forgetting to eat and stock up is noted. Emerging eating disorders are linked to memory disorders and spatial and temporal disorientation.
The major risks associated with food are undernutrition, weight loss (a person can be undernourished without being lost weight) and false roads. The challenge is to increase energy and protein intake without increasing quantities.
When a sick person is detected with a decreased appetite, weight loss or undernutrition, the challenge is to increase energy and protein intake without increasing quantities to ensure that the person will eat all the dishes offered. This is the principle of enrichment. It may be appropriate to carry out a check-up with a speech therapist or physiotherapist.
Toilet/ Dressing
When the toilet becomes difficult to perform, it is often complicated to set up a help for the sick person because one enters his intimacy. The intervention of a family member for this type of care should not be trivialized. Regardless of your relationship with the sick person, you will certainly never have had access to your loved one's body in this way. It will affect your relationship. This is why the intervention of a professional is often desired to accompany the toilet. Take time to explain. Toilet should be presented as a pleasure and not a constraint... If the word "toilet" frightens the person, it may be appropriate to use other formulations such as "I will take care of you", "we will make you beautiful". Time should be taken to explain to the sick person the process of washing.
It can happen that the sick person expresses aggressiveness during the toilet, it can be related to fear and discomfort. It is important to try to understand what type of toilet is less stressful for the sick person: in the sink, shower, bath, bed ?
While it is still possible; you can offer the person to choose how they want to dress. However, putting the person in front of a too important choice risks putting him/her in a situation of failure, so it is preferable to offer only two possibilities.
The choice of clothes is important for self-image and comfort. If the person has clothes where they feel tight, uncomfortable, they can be disturbed all day long.
(France Alzheimer's)
The Night
The bedtime should be ritualized to help the person understand what is expected and allow him/her to surrender to sleep.
Anticipate bedtime
Anxiety is often increased in the late afternoon or early evening. It is related to nightfall and fatigue accumulated throughout the day. In order to facilitate the bedtime stage, it is important to avoid asking the sick person to perform too complex tasks at the end of the day and to offer him/her a relaxing time before going to bed.However, in order for the night to be dedicated to rest, it is also important to preserve activities during the day (walking, artistic activities, etc.).
Preventing nighttime wandering
Night is a time when a person with Alzheimer's disease or a related disease is most likely to put themselves at risk. It is not uncommon at night for feelings of abandonment and anxiety to drive the person away from a place that has become foreign.
She may also think, when she wakes up successively, that the time has come to get active, have lunch, get dressed... or even suppose, when she sees it when she wakes up, that it should normally be daylight and worry about it. (France Alzheimer) In these different situations, the person gets moving and sometimes tries to get out of the house. To avoid this, you have to try to understand why the person gets up at night: often the person may be hungry or thirsty, to prevent them from moving, you can have food or drink near the bed; they may also want to go to the toilet, so it is better to leave the light in the bathroom or hallway so they can spot the place more easily. Driving is a complex activity that requires rapid reactions, alert senses and immediate decisions. For a person with Alzheimer's disease, driving inevitably becomes difficult.
In all cases, when the decision to stop driving is made jointly by the doctor and family, you should never go back.
Outgoing
Fearing the behaviour of the sick person or the judgment of others, caregivers are sometimes reluctant to continue to organize outings outside, yet when they are still possible, they are beneficial. It is important to prevent the sick person from letting himself or herself be swept away by apathy. It is important that she keeps, if possible, a regular rhythm of activity, to maintain herself both physically and morally. Walking, jogging, football, cycling, swimming... any physical activity is good as long as the sick person enjoys it... The benefit is twofold: keep fit and relieve stress. In addition, during each outdoor outing, the sick person can be encouraged to look, feel, listen and touch. The purpose of the outings is really to share a time of pleasure with the sick person and to prevent him/her from falling into a withdrawal attitude.

*Amyloid plaques: an amyloid is abnormally secreted by neurons. It gradually settles throughout the brain, covering neurons and their extensions. At an advanced stage of the disease, the deposits of this substance aggregate with the already affected neurons to form "amyloid plaques".
* Neurofibrillary degeneration: accumulation inside the neurons of pathological filaments, consisting of a protein called Tau and leading to the progressive death of neurons. (France Alzheimer)
MEDICAL RESEARCH IN THE WORLD.
There is a lot of research underway to better understand Alzheimer's disease, detect it early and treat it.
Currently, the diagnosis of Alzheimer's disease is based on neuropsychological assessment and brain imaging tests. But this method would only detect half of all patients. However, recent studies indicate that the first neural disorders may be present up to ten years before diagnosis. One of the challenges is therefore the development of an assay for biological markers in the blood. Trials are also underway to test high-performance brain imaging techniques;
At the same time, epidemiological studies aim to identify risk factors by studying a large number of people for many years.
In neuroimaging, researchers have developed radiotracers to detect in vivo amyloid plaques in patients. Several teams are now working on the development of radiotracers to visualize Tau.
A research challenge is to develop and identify new biomarkers. These should be easily usable (e. g. blood testing techniques) and reliably indicate the presence of the disease. Such biomarkers will be essential tools for the early diagnosis of Alzheimer's disease and should allow for better management of people with the disease. (France Alzheimer)
Developing innovative therapeutic strategies
Therapeutic research is very active in the field of Alzheimer's disease. Currently, some 120 therapeutic molecules are in the testing phase. Some aim to block the accumulation of amyloid peptides while others try to block the abnormal phosphorylation* of Tau proteins, which causes neurofibrillary degeneration. Researchers are also very active in the development of immunotherapies. The objective is to activate the patients' immune defences to destroy amyloid plaques...
Phosphorylation: it is a fundamental chemical reaction in biology, regulating the function of very many proteins. In Alzheimer's disease, the hyperphosphorylation of the Tau protein seems to favour its aggregation and the formation of neurofibrillary degenerations.
To go further: immunotherapy
Immunotherapy is one of the therapeutic hopes against Alzheimer's disease. This strategy consists of using antibodies to suppress the accumulation of amyloid peptide. The first trial of a vaccine against the amyloid peptide showed a high rate of complications (inflammation of the meninges and brain) following treatment. However, patients who responded to treatment saw a significant decrease in the amount of amyloid deposits in their cerebral cortex. At the same time, at the clinical level; improvement in neuropsychological evaluation has also been observed.
Based on these results, many research teams are pursuing work to develop appropriate vaccination techniques.
Today, 3 million French people are directly or indirectly affected by Alzheimer's disease, including more than 850,000 sick people. With nearly 225,000 new cases diagnosed each year, the disease is progressing, if nothing changes, France will have 1,275,000 sick people in just 8 years.
Despite the extent of Alzheimer's disease, we remain poorly informed about this pathology, which is still poorly known, poorly perceived and insufficiently managed. (France Alzheimer)
Prevention
The food path
Different studies have been conducted on the impacts of a certain diet in the prevention of Alzheimer's disease. Several observations were made in particular concerning the Mediterranean diet, which includes the following Several observations were made in particular concerning the Mediterranean diet, which gives priority to the consumption of fish, fruit, vegetables and olive oil. For example, subjects who consume fish two or three times a week have been shown to reduce the risk of cognitive decline. These are interesting prevention approaches but they still need to be confirmed by more detailed long-term studies.
The physical and intellectual activity approach
In the context of prevention, we talk more about physical activity than sports activity.It is of course advisable to maintain physical activity at all ages of life, whether it is walking or simply climbing stairs instead of systematically taking the elevator. While this is a good way of prevention, it is not specific to Alzheimer's disease.
Concerning the so-called "intellectual" activities, there are demonstrations in particular. These are interesting prevention approaches but they still need to be confirmed by more detailed long-term studies.
The physical and intellectual activity approach
In the context of prevention, we talk more about physical activity than sports activity. It is of course advisable to maintain physical activity at all ages of life, whether it is walking or simply climbing stairs instead of systematically taking the elevator. While this is a good way of prevention, it is not specific to Alzheimer's disease.
Concerning the so-called "intellectual" activities, there are demonstrations in the area of the city of Montreal.It is of course advisable to maintain physical activity at all ages of life, whether it is walking or simply climbing stairs instead of systematically taking the elevator. While this is a good way of prevention, it is not specific to Alzheimer's disease. Concerning the so-called "intellectual" activities, there are demonstrations in favour of workshops stimulating memory, logic or reflection, which would reduce the risks. But here again, scientific trials are still ongoing:
Alzheimer's Disease International (36 million patients worldwide), In Europe, it affects more than 1 million people (mostly women) in France and 1.2 million in the United Kingdom. In the USA it is a national cause and affects more than 5 million patients, ½ million deaths per year. The US federal budget to deal with this is constantly increasing and amounts to more than USD $220 billion per year (Alzheimer's Association). The global annual global cost of Alzheimer's disease and dementia (brain aging) is estimated at USD 605 billion, or about 1% of global GDP in 2013.
The most famous victims who died are: Charles BRONSON (American, film actor), Louis FERAUD (French designer and couturier), Rita Hayworth (American actress), Charlton Heston ( American, film actor), Jack Lord (American, film actor), Ronald Reagan (US President, 40th), Peter Falk alias colombo inspector (American actor), Annie Girardot (French actress)
B/ Le soutien aux droits de la femme.
We believe in women rights and equality. GNF will work as much as possible, to improve, help and contribute to achieve women rights, equality and empowerment.
- Legal advice,
- Business and entrepreneurship
- Tuitions
- Short terms education,
- Training….
C/ Youth and education
We will provide a material and financial support, to selected projects for youth and education. Such as orphans, school, recreational aeras, etc…
- Tuitions
- Books, clothes, medicines, etc…
- Professional insertion…
D/ An analysis of economic life in Cameroon and/or in the world.
We will publish a monthly review, or analysis of the economy, in Africa and the rest of the world. Our team will select a personality of the world, to express it views, on a specific topic of the economy.